The knee is a fickle joint. On one end it is the cause for many major injuries, ranging from anterior knee pain, to ACL reconstruction. And on the other end, there has been a push for “ACL Injury Prevention” programs, largely aimed at the female demographic, but the way the Eagles have started their 2013 pre-season year, it seems someone needs to take notice of this as well.
But does the knee just need to succumb to the whims of eventual injury? With over 200,000 ACL injuries seen annually, and of these injuries, 100,000 are reconstructed, at approximately $50k to $60k in surgery to fix the problem, you can see that this is a large investment for health purposes and return to play demands as well. (1)
[youtube=http://www.youtube.com/watch?v=cKKHSAE1gIs]
Of the dancing population, and I’m not just talking about flash mobs, females need to pay special attention to this, not only for biomechanical reasons in regards to the hip to knee angle (or the Q-Angle), but also because many more females go under the knife at a statistically higher rate than their male counterparts in those who do get injured. (2)

Looking at the research found in dance and sports medicine points us to the direction of avoiding knee hyperextension to limit the amount of bone on bone contact, and spending time increasing the amount of appropriate force absorption through the menisci and/or muscles surrounding the knees (and hips).
With the combination of single leg hops, turns, and precision techniques, often found in modern and classical dances, there are decelerative and shock absorbing affects found in the ankles, knees, and hip anatomy. Further, with the amount of ground reaction forces transferred from the ground to the ankle, up through the knee and finally through the hip, it is prudent to understand that the knee is whim to the forces absorbed or the passive ranges of motion in the joint above or below it.
[youtube=http://www.youtube.com/watch?v=uQ7bxim_MXc]
Theoretical Approach
Simply put, any degenerative changes seen at the knee could be prevented through a three pronged approach. Assess for 1. lack of ankle dorsiflexion and 2. hip motion (whether flexion, extension, or external and internal rotation). After determining the range of motion and accompanying functionality of the hip and ankle musculature, 3. proper neuromuscular training, whether dynamic warm-up drills, reactive work, or stability/isometric exercises, will help reintroduce appropriate patterning for knee injury prevention.
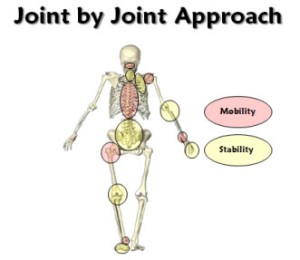
One area that is glossed over by in the Joint by Joint Approach (JBJA) in regards to the knee is that it assumes that the knee may be susceptible to issues if there is a general lack of mobility in the ankle or hip. However, in many dancers, either through congenital predisposition, or through adaptations through training, exhibit a greater than normal range of motion in the ankle joint in both dorsiflexion and plantarflexion. What does ankle dorsi- and plantarflexion have to do with the knee? Referring to the above picture, quite a bit in fact.

Does this dancer need more mobility? I’d venture to guess not – either more stability work needs to be introduced (up the chain), and possibly even soft tissue maintenance of the ankle joint to prevent any issues from occurring up the kinetic chain as well.
Further, genu recurvatum, or knee hyperextension, found by a static postural assessment, will often present an anteriorly tilted pelvis, along with lordosis of the spine, much like this dancer presents.
Approaching the Bees Knees
So the patterns for injury that are unique to the knee definitely make it an even more unique creature in dancers. What interests me most in the knee in dancers is the approach many take towards knee issues. More often than not, there is stretching of the hamstrings, not much care taken for strengthening the posterior chain or maintenance of stability, and icing or compression of the knees (in breakdancers at least) to prevent injuries after sessions and to warm-up before dancing, respectively.
Before delving into the various issues with this approach, here is the bees knees on the knee’s anatomy. (See what I did there?)

Muscles of the Knee Joint
Extensors
- Quadriceps
- rectus femoris
- vastus lateralis
- vastus intermdius
- vastus medialis oblique
Flexors
- Hamstrings
- semimembranosis
- tendinosus
- biceps femoris
- Sartorius
- Gracilis
- Gastrocnemius
Medial Rotators (Internal Rotation)

- Semitendinosus
- Semimembranosus
- Sartorius
- Gracilis
- Adductor magnus
Lateral Rotators (External Rotation)
- Biceps femoris
- Rectus femoris (when exhibiting anterior pelvic rotation)
- Adductor longus
- Pectineus (after 90° of hip flexion it becomes hip internal rotator
Femoral Stabilizers
- Adductor Magnus
- Biceps Femoris
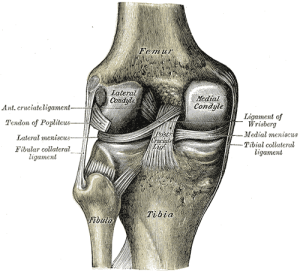
Ligaments of the Knee Joint
- Anterior Cruciate Ligament
- Posterior Cruciate Ligament
- Medial Cruciate Ligament
- Lateral Cruciate Ligament
(The above does not even represent the hip musculature such as gluteals, obturators, etc.)
Despite the vast amounts of knowledge gained osmotically through your eyes as you memorize the above three pictures, simply knowing the anatomy may not necessarily alleviate any knee issues. Applying the joint by joint approach will point us to look at the hip region, and utilizing various movement assessments, the first aim is to determine if the pelvis needs repositioning, before “fixing” any knee issue. After neutrality is observed through a re-test of the assessment, and the knee still presents issues, then we can begin to look more specifically at knee pathologies and problems.
Why should you look at the hip to find the root of the knee problem?
As I’ve alluded to, knee stability is often found through control of the hip muscles. Thomas Myers has introduced the idea of the kinetic chain, and from a fascial and muscular point of view, the hips control the knee. (3) To use one muscle as an example, if the glute max facilitates external rotation of the hip, the femur will have to naturally follow along and externally rotate. If the femur externally rotates, the next natural step will be for the knee to move laterally or externally rotate as well.
So whether you believe the knee is a hinging joint or a condyloid joint with secondary motion for external and internal rotation, however small it may be, it is at the mercy of the hips, much like I am at the mercy of Shakira’s hips in any of her music videos.

When speaking strictly about dancers, there comes about several questions. Namely, how do you dance? Do you ever purposefully land on the knees? If there is purposeful contact with the ground, is there a way to protect the knees? What do your spins, turns, and jumps look like?
Suffice to say, there is a lot of individualistic movement patterns to take into account, despite the vast amounts of literature pointing to knee pain strictly as a cause of degenerative or repetitive movement adaptations at the hip or even ankle level.
###
Much like Dre said, “Til the next episode…”
Keep it funky,
MA
REFERENCES
1 – http://orthosurg.ucsf.edu/patient-care/divisions/sports-medicine/conditions/knee/anterior-cruciate-ligament-injury-acl/#.UhcjbqUwDao
2 – http://www.medscape.com/viewarticle/780288
3 – Prins, Maartin, and Peter Van Der Warff. “Females with Patellofemoral Pain Syndrome Have Weak Hip Muscles: A Systematic Review.” Australian Journal of Physiotherapy 55 (2009): 9-15. Web. <http://ajp.physiotherapy.asn.au/AJP/55-1/AustJPhysiotherv55i1Prins.pdf>